AFR Tracker
Cardiolund AFR Tracker
Why can we not properly diagnose and treat the most common arrhythmia?
Atrial fibrillation (AF) is the most common abnormal heart rhythm, and is considered to be the resulting end state of several possible mechanisms. The risk of developing AF increases with age and with other risk factors such as diabetes, high blood pressure, and underlying heart disease. A heritable component may also be involved. AF may occur in episodes lasting from minutes to days, or be of permanent nature. It may cause no symptoms, but can be associated with symptoms of heart illness, including palpitations, chest pain, fainting, etc. AF can result in a reduction of cardiac output or formation of blood clots in the heart, and the risk of stroke is therefore significantly increased in individuals with AF. A number of treatment options are available, but the efficacy of each is relatively low.
With limited possibilities to understand the cause of the disease in the individual patient, there are, as a consequence, also limited possibilities to predict the outcome of different therapies and select the best one of those for the individual patient.
In order to learn how to better diagnose and treat patients with AF, we need to be able to 1) observe the difference between different patients, i.e., measure the disease state, and 2) quantify the effect on the disease state caused by interventions.
When studying the detailed ECG signal patterns in AF patients, a considerable variation between individuals can be observed. And, it has been shown that these patterns can be altered by, e.g., drugs and autonomic manoeuvres. With a conventional approach to selecting an AF treatment strategy for the patient, the signal patterns are not taken into account. There are two simple explanations for leaving out this important data: The interpretation of the AF pattern is not fully understood, and the AF pattern cannot be quantified manually.
The atrial fibrillatory rate (AFR) is useful
The atrial fibrillatory rate (AFR) is a feature that can be calculated for ECG signals from patients with AF. With AFR, you can measure differences between patients with AF, and you can quantify the effect on the atria of different interventions, such as anti-arrhythmic drugs or autonomic manoeuvres.
The atrial fibrillatory rate can be seen as a window into the atria, revealing the state of the atria, using standard ECG measurements and computer algorithms. AFR measures the activation rate of the atria, and is an index of the intra-atrial organisation.
Scientific studies have shown that patients with a lower AFR is more likely to spontaneously convert to sinus rhythm, and they are also more likely respond to treatment of any kind (DC conversion, anti-arrhythmic drug, and ablation).
AFR is used to measure differences between individual AF patients, and between groups of AF patients, such as responders and non-responders to treatment, short and long duration AF patients, and patient groups with different genotypes.
AFR has also been used to evaluate the effect of novel anti-arrhythmic drugs in collaboration with some of the worlds largest pharmaceutical companies.
In such studies, AFR shows how and to which degree the patients not converting to sinus rhythm responded to the treatment. To quantify the effect of different dosages, to measure non-invasively how long time the drug is active before the effect is decaying, and maybe most importantly, to understand what happens between the drug intake/infusion until conversion or peak effect of the drug are possibilities presently only possible using AFR.
For more details on scientific studies related to AFR, see the full publication list at https://cardiolund.com/references.
Improving diagnosis and treatment using the AFR Tracker
Cardiolund has developed the AFR Tracker software, which automatically calculates AFR, and measures changes in AFR, for a set of ECG signals from a patient or patient group.
The software also calculates a number of statistical measures related to AFR which are useful for evaluation of AF treatment strategies.
There is a wide range of possible research and clinical applications of AFR, including the possibilities to investigate:
- If AFR can predict treatment outcome, by comparison between responders and non-responders to treatment or other interventions.
- The effect on the atria of a treatment option, and evaluate the effect of different dosages, by comparison between AFR before and after treatment.
- The mechanisms of AF, by analysis of spontaneous and diurnal variations, or autonomic responses in AF.
- The entire response and recovery of the atria during drug treatment, by trending the AFR from minute to minute.
- AF genotypes by using AFR and AFR drug responses as phenotypes of AF.
Example use cases
One important application area for AFR is the prediction of spontaneous AF termination, or termination induced by DC conversion, anti-arrhythmic drugs and ablation procedures. Numerous scientific studies have been performed on these topics. A summary of this work is provided in: Atrial fibrillatory rate in the clinical context: natural course and prediction of intervention outcome by Platonov PG, Corino VD, Seifert M, Holmqvist F, Sörnmo L, Europace. 2014 Nov;16 Suppl 4, p110–119.
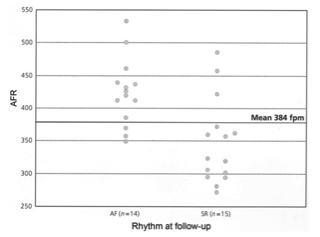
An example in this application area, is the study of sinus rhythm maintenance after DC conversion that is described in Atrial fibrillatory rate and sinus rhythm maintenance in patients undergoing cardioversion of persistent atrial fibrillation by Holmqvist et al (European Heart Journal (2006) 27, 2201–2207). The study found that among patients with an AF duration less than 30 days, sinus rhythm was better maintained in the group with a lower AFR, see figure below.
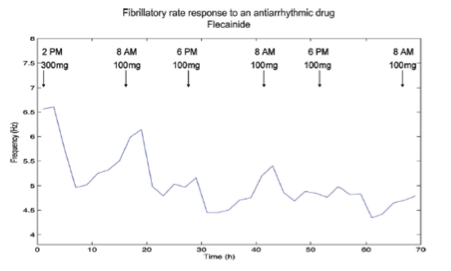
Another example is the study reported in the paper Analysis of surface electrocardiograms in atrial fibrillation: techniques, research, and clinical applications by Bollmann et al (Europace. 2006 Nov;8(11):911–26). Herein, the effect of oral treatment with the anti-arrhythmic drug Flecainide is followed for 3 days after initiation. The figure below shows how both the individual effect of each dose, as well as, the total effect over several days can be evaluated. AFR was in this case calculated from Holter recordings using Cardiolund’s AFR Tracker algorithms.
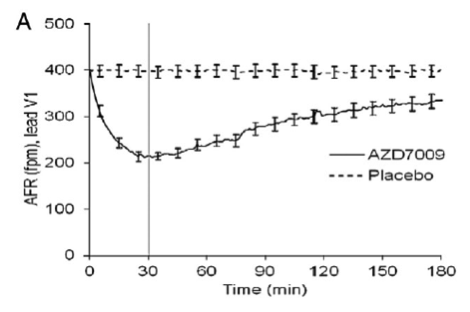
A third example is the study reported in the paper Decrease of the atrial fibrillatory rate, increased organization of the atrial rhythm and termination of atrial fibrillation by AZD7009 by Aunes-Jansson et al. (J Electrocardiol. 2013 Jan-Feb;46(1):29–35). Herein, AFR trending with software from Cardiolund was used to evaluate the effect of a novel anti-arrhythmic drug. Several measures including AFR (per second or per minute), HR, time to peak effect/conversion, lowest AFR before conversion, and increase of AFR per minute after peak effect are possible to calculate, see figure below.
How AFR is calculated
The AFR calculation requires that the patient's ECG is recorded during, or contains, an AF event, and that the f-waves can be clearly seen in the signal. Lead V1 is the most commonly used signal for AFR calculation but other standard ECG leads as well as Holter leads have also been used.
The Cardiolund AF Tracker software is an add-on software to the Cardiolund ECG Parser, which provides a very detailed description of the ECG signal.
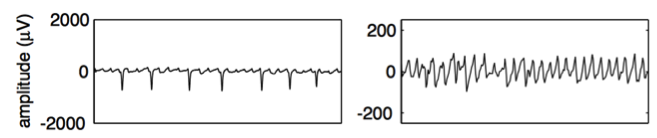
The AFR Tracker first removes the ventricular activity from the ECG, producing a residual ECG signal. An example residual ECG is shown in the figure below, with ECG lead V1 to the left and a rescaled residual ECG to the right.
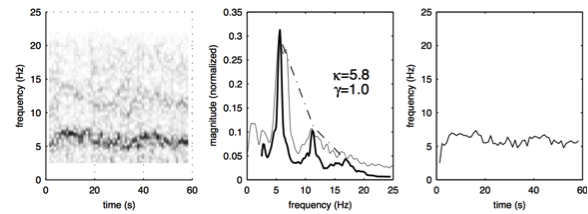
Next in the AFR Tracker, sequential time-frequency tracking is applied to the residual ECG (see left panel of figure below) resulting in a frequency trend describing the atrial activation rate over time (right panel of figure below). Frequency is here in Hz but is normally converted to fibrillations per minute (fpm) by multiplying with 60.
System integration
The AFR Tracker can be applied to signals from all standard ECG systems. The software is available for system integration in a server based solution through a pre-compiled binary link-library.
The AFR Tracker is meant for integration with other software that allow users to display and browse analysis results. The software does not include a graphical user interface, nor does it provide features for data capture and storage management.
The software can be customised and extended to provide different types of analysis reports, but it can also serve as an analysis platform supporting your device’s own user interface. The analysis reporting can be adapted to fit your specific requirements, e.g., localisation to specific languages.
Cardiolund provides documentation for easy system integration, and also the supplementary documentation as needed for certification of your product.
For more information on the AFR Tracker product, please contact us.